Which came first – Bone graft or Membrane?
What materials exist, and how do they compare?
Before implant restoration became widespread, Guided Tissue Regeneration (GTR) procedures were offered, which utilised dental membranes to exclude gingival tissue from occupying a periodontal pocket giving bone and periodontal tissues the space and time to regenerate. The first barrier membranes (expanded PTFE AKA GoreTex) created the required healing compartment, yet required a second procedure to remove. These materials were associated with a high incidence of dehiscence and infection, prompting the development of bioresorbable matrix barriers by Gottlow and co-workers in the late 1980s.
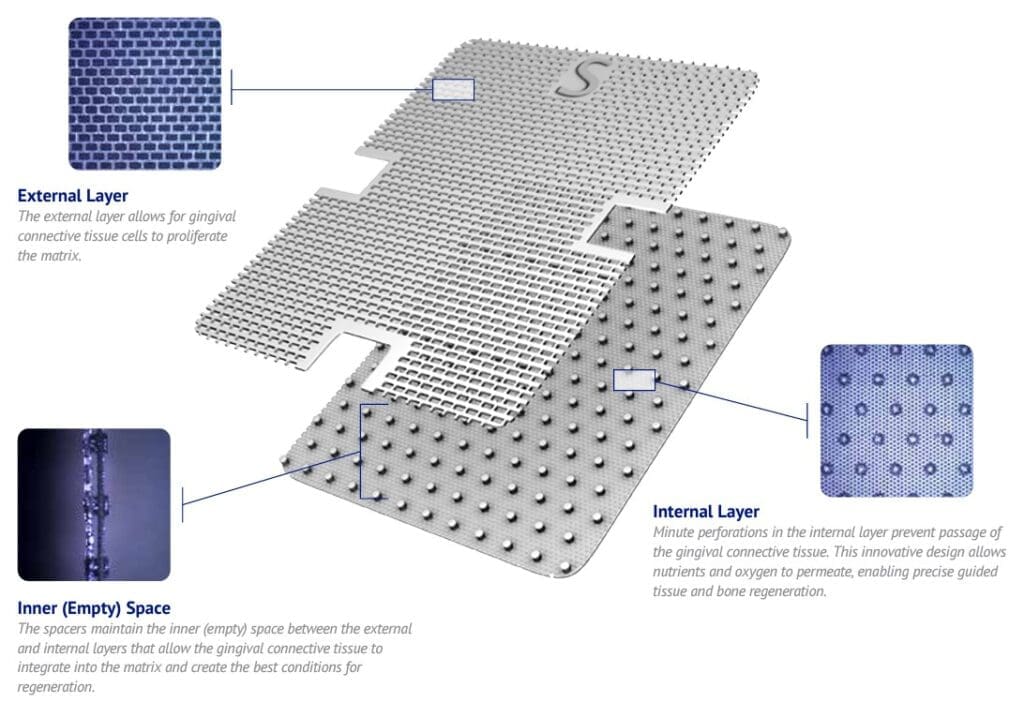
Image shown:
Guidor bioresorbable matrix barrier
Guided Bone Regeneration (GBR) membranes
As Dental Implant restoration increased, the materials used for GTR were revised to meet the needs of GBR, especially the requirement for them to be resorbing. Guidor bioresorbable matrix barrier (as shown) was an early example of a resorbing GTR barrier adapted for GBR procedures. Despite excellent clinical results, the technical challenge of production limited its supply, creating the demand for alternative resorbing materials. Resorbing collagen appeared as an alternative at the same time as general dental practitioners were emerging as alternative providers to specialists such as periodontologists and oral maxillofacial surgeons, promoting its uptake.
All barrier membranes require surgical skills such as flap management and fixation, which were not well taught in the general dental community. Additionally, one of the challenges when using collagen membranes is the collapse into the defect, which occurs if a space-filling material is not used underneath. These factors led to the emergence of proprietary bone graft scaffolds and bone void fillers, which gained popularity in GBR alone and in combination with barrier membranes.
Today, due to the development of more advanced proprietary bone graft materials, many implantologists report the regeneration of excellent new bone without the need for a dental membrane. One such material is Powerbone Dental Putty.
WHEN IS A BARRIER MEMBRANE NEEDED?
Barrier membranes carry three key functions:
- To create a healing space for bone and periodontal tissue.
- To reduce micromovements inherent in particulate bone grafts, because movement between particles delays healing.
- To help exclude soft tissue invasion during the healing phase.
WHAT TYPE OF DENTAL MEMBRANES EXIST TODAY?
Dental barrier membranes can be resorbable or non-resorbable. Non-resorbable membranes are better at creating space, yet typically require a second procedure for removal, with the disadvantages of time and trauma. Fully resorbable barrier membranes offer the advantages of a single procedure in exchange for reduced space maintenance.
Non-resorbable Dental Membranes
Titanium Mesh
Ti-mesh predictably maintains space making it ideal for the reconstruction of the severely deficient alveolar ridge. Ti-mesh can be shaped to match the defect and allows an unimpeded blood supply from the periosteum due to its holes (pores). Standard Ti-mesh is available in rectangles, which are ideal for delayed (two-stage) regeneration and implant surgery. Standard Ti-Mesh is fixed in place with stainless fixation screws or tacks.
Sometimes titanium mesh is used to reinforce a PTFE (poly-tetrafluoroethylene) polymer membrane, such as the original GoreTex brand. This was shown to be susceptible to microorganism transfer, especially so after exposure to the oral environment (dehiscence), which increases when wound closure is sub-optimal. High-density polymers can be used instead of e-PTFE as they offer similar handling and application yet resorb fully, removing the need for a second removal procedure. See Powerbone Polymer Membranes
Resorbable Dental Membranes
Fully resorbing dental barrier membranes can be distinguished by their origin and the time frame in which the barrier function is maintained.
Animal origin

Collagen is a protein that makes up the structure or framework in connective tissue, skin, tendons, bones, and cartilage. The collagen used in resorbable dental membranes is sourced from the pericardial or peritoneal areas of pigs or cows. Pericardial collagen presents a higher mechanical strength than peritoneal collagen. The original bovine peritoneal collagen (Geistlich Bio-Gide) is less stiff and more prone to collapse into the wound, promoting the development of extended-function collagen materials.
Function time and cross-linking.
Functional resorption time is different from complete resorption time, as non-functional remnants will remain long after the barrier function is compromised. Because native collagen is a protein, it can resorb quickly, and if exposed to saliva, this dissolution can be rapid. The resorption time directly impacts function and is a limiting factor for the use of basic native collagen membranes in dental bone graft procedures. It is one reason Geistlich recommends two layers for its Bio-Gide despite the obvious disadvantages this brings.
Methods to extend the resorption time of collagen membranes include chemical and physical processing. Processing with chemicals such as glutaraldehyde successfully extends the resorption time for a collagen membrane. Unfortunately, products cross-linked with glutaraldehyde increase inflammatory response and are reported to be toxic in higher concentrations.
Cross-linking via process development
For these reasons, methods to physically modify the collagen were developed, such as dehydrothermal (DHT) treatment. When applied to porcine pericardial-sourced collagen, DHT treatment produces a membrane that exhibits high tensile strength, resistance to degradation, and reduced inflammatory responses. One such material is T-Gen (also called Ossguide). Another similar material with longer functional performance is available under the name Ti-oss GUIDE.
Polymer (synthetic) origin
The polymer materials of polylactic (PLA), polyglycolic (PGA), and poly(lactic-co-glycolic) acid (PLGA) are widely used in various medical applications, e.g. as biodegradable implants in surgery, as raw materials for wound closure stitches or as carrier substances for the delivery of pharmaceuticals. They present excellent biocompatibility and adjustable degradation rate and are non-toxic in humans. (1) and were the first resorbable materials used for GTR and GBR with high tensile strength and excellent space maintenance.
ENHANCED FUNCTION, DIFFERENT CHARACTERISTICS
One or two layers?
Clinicians familiar with PTFE will find the double-layer Powerbone Resorbing Synthetic familiar. Clinicians transitioning from Resorbable Collagen, such as Ti-oss Guide, should consider the single-layer version more familiar.
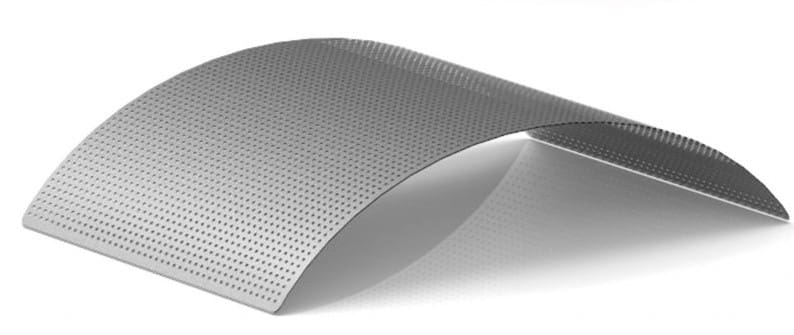
Preparation and Fixation – Thermo moulding.

Resorbable synthetic membranes can be thermo moulded before application, making them more able to match the bone architecture. When used in this way, resorbing polymer membranes create better space and are more substantial barriers than resorbing collagen. Powerbone Resorbing Polymer Membrane can be placed in a warming cabinet or the primary plastic container immersed in warm water before use. Fixation is recommended to ensure a snug defect continuity. Simple membrane tacks are available in titanium and absorbing polymer types.
In summary
| COLLAGEN | RESORBING POLYMER | PTFE / TI-REINFORCED |
| Mixed-density resorbable synthetic polymer sheets are produced by the plasma spray process. | Mixed-density resorbable synthetic polymers. | Polymers or reinforcement with titanium mesh. |
| COLLAGEN FEATURES | RESORBING POLYMER FEFATURES | PTFE / TI-REINFORCED FEATURES |
| Porous and biocompatible Good tissue integration. Fast vascularisation Good adhesion. | Lab consistency less variation. | Lab consistency, fewer variations. Excellent space creation. Do not collapse. |
| COLLAGEN LIMITATIONS | RESORBING POLYMER LIMITATIONS | PTFE / TI REINFORCED LIMITATIONS |
| Function time can be limited. Disappear quickly when exposed. | Less elastic (warm before use) Less adherent Fixation is recommended. | Non-adherent and unstable. Fixation is mandatory. Limited porosity. Higher incidence of exposure. Removal is mandatory (delays healing) |
BROWSE AND PURCHASE
Resorbable and non-resorbable membranes and fixation tools can be browsed and purchased online from Regen store HERE.
References
- Sharma. PLA/PLGA nanoparticles prepared by nanospray. Journal of Pharmaceutical Investigation volume 49, pages 405–426 (2019.