Post extraction alveolar bone loss occurs first in width and then in height. Anteriorly this impacts aesthetics whilst posteriorly it challenges optimal implant placement and loading. Bone atrophy affects medullary bone first meaning resorbed sites present more cortical than non-atrophied sites – important for implant stability which relies heavily on cortical bone contact.
Patients presenting with bone atrophy are typically edentulous or present with dentures of poor prognosis. Increasingly, atrophy is seen around failing implants that present for revision.
Implant expert, Dr David Morales proposes two treatment strategies:
Reconstructive approach.
New bone is regenerated to support a standard implant in a three-dimensional position placed at a second stage. Regenerated bone will remodel around the implant according to the loads placed upon it (following Wolff’s law). A fully resorbing graft (ie Powerbone Dental Putty) would deliver maximum bone in such a case.
Anchorage approach.
A bony site is selected to place a special fixture capable of supporting the prosthesis using existing bone to create stability. Regenerative techniques are employed later to add volume using a slow turnover material such as a Biphasic. Implants for anchorage approaches are either very long or very short designs.
For the atrophic maxilla – VERY LONG IMPLANTS
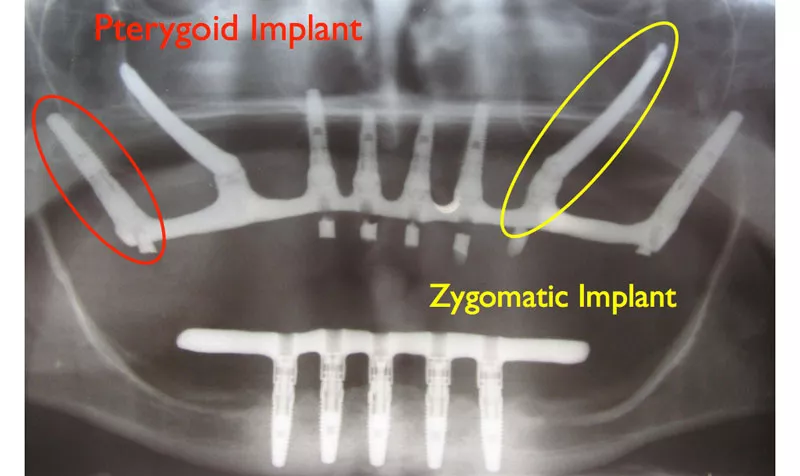
Very long implants can be supported by bone in either the pterygoid process of the sphenoid bone, at the base of the skull, or the zygomatic bone which forms the prominent portion of the cheek. To locate effectively, Pterygoid and Zygomatic implants need to be considerably longer than conventional implants at c55mm.
An alternative option is to place a fixture of 18-25mm across the sinus with apical fixation in the nasal cortical bone. Trans-Sinus Implants, such as DM Plus from Bioner Spain, range in length from 18mm to 25mm. All Pterygoid, Zygomatic and Trans Sinus implants require an angled restoration.
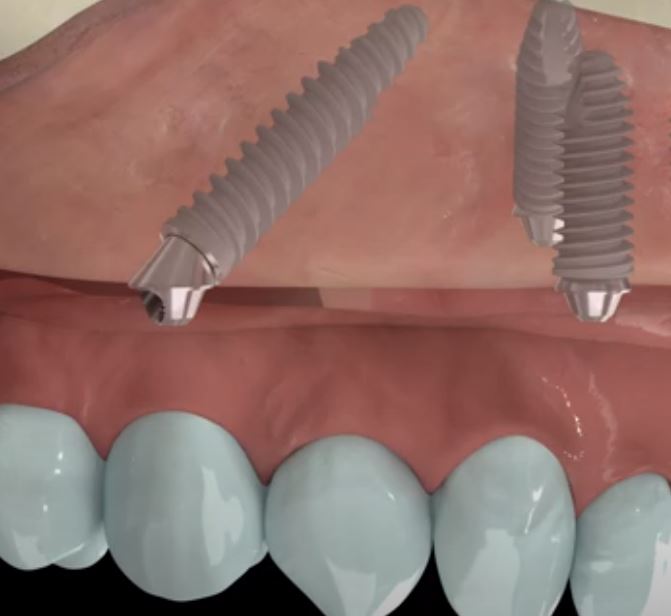
For the atrophic mandible – VERY SHORT IMPLANTS

Research tells us that 95% of implant load is concentrated on the coronal 4 to 5 mm of any dental implant – the part anchored in cortical bone. As such implants of 4, 5 or 6mm length placed directly into the mandible suit patients who seek a quick, stable solution with low morbidity.
Short DM from Bioner Spain.
Short DM is a sub-6 mm fixture designed for limited bone sites such as the atrophic mandible. The mechanical stability of Short DM is enhanced by a design which utilises:
- A cylindrical profile for increased bone-to-implant contact.
- The best-roughened surface for increased surface area.
- The Bioetch™ surface is formed by a patented double etching process without sandblasting which completely eliminates impurities which are shown to reduce healing and slow integration.
- A wide shoulder which engages the flattened crest created by the ridge flattening drill.
Restoration and long-term success of ShortDM are assisted by:
- A polished 2mm collar for gingival sealing and reduced marginal bone loss.
- An indexed conical connection which minimizes implant and abutment micromovement.
- Standard restorative components can be selected from the TopDM catalogue.
Safe and Secure™ placement near critical structures.
Drilling based upon Neurosurgery
Regular cutting drills near the inferior dental nerve constitute a high risk. Based on the neurosurgical speciality (in which precision and safety are especially critical) Bioner presents the innovative Secure™ drilling system:
->Diamond-coated drills enable close work in critical areas at reduced risk.
->A ridge flattening drill creates a ledge to engage the matching wide shoulder of Short DM.
Short DM – The innovative, secure system for the atrophic mandible.
Read more about ShortDM here.