Dental Implant restorations even with high-quality dental implants can present for revision. Peri-implantitis is one of the main concerns as is sclerotic bone associated with fibrous encapsulation of some types of non-resorbing processed graft materials.
Peri-implantitis.
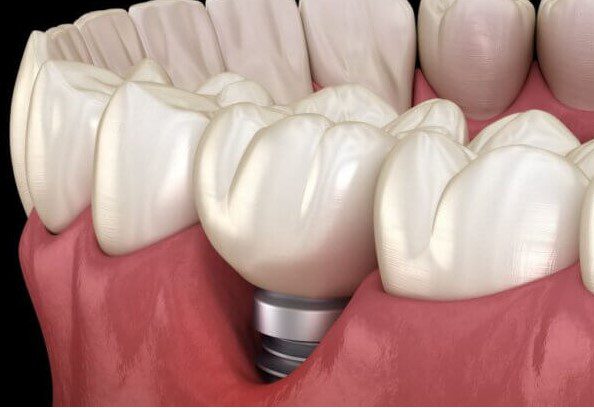
Peri-implantitis is a plaque-associated condition around an implant that results in a breakdown of the supporting tissues. Peri-implant-affected sites exhibit bleeding on probing and/or suppuration with increased probing depths and/or recession and can progress to bone loss. If untreated, the disease progresses in a nonlinear pattern and leads to implant loss (1).
Sclerotic Bone
Dr Greg Steiner, D.D.S., M.S (California) – an expert in tissue engineering reports on numerous cases of a peri-implant inflammation associated with residual graft particles, which results in sclerotic bone seen radiographically. This bone loss is complicated by creating a defect adjacent to the implant that becomes a secondary infection. Dr Steiner recommends avoiding cadaver-derived mineralised bone grafts, especially so adjacent to an implant surface, as fibrous encapsulation can result with reduced bone-to-implant contact.
NiTi decontamination brushes.
The most important preparatory steps before regenerating bone is to mechanically (sometimes chemically) decontaminate the implant surface completely and remove granulation and unhealthy hard tissues from the surface and surrounding site.
NiTi decontamination brushes provide significantly greater reductions of initial PD and stable bone levels compared with plastic curettes or air-abrasive devices (2) and are an efficient and intuitive way to remove plaque, calculus, and other foreign body material from the implant surface.
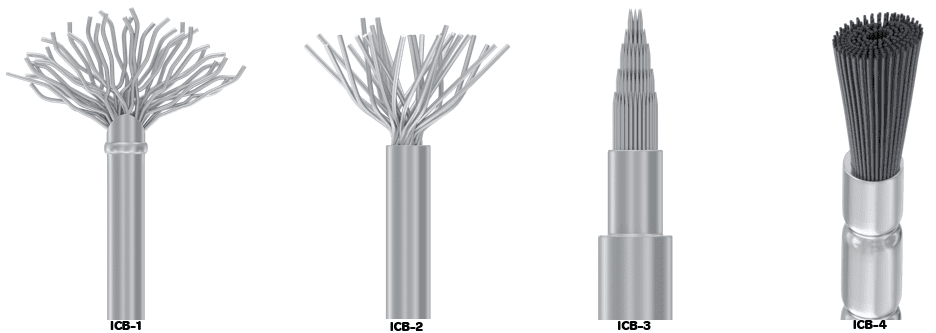
What is NiTi and what are they?
NiTi stands for Nickel Titanium and refers to the filaments used on the debridement brushes. NiTi also known as nitinol, is a metal alloy of nickel and titanium, where the two elements are present in roughly equal percentages. For Dentistry, NiTi Brushes are available in a variety of types such as:
Using NiTi brushes to debride an implant.

Each brush is attached to the handpiece and is moved rotationally along the circumference of the implant. Using a speed of 500-1000 rpm and a torque of 50Ncm with irrigation each brush adapts closely to the implant architecture due to its flexibility to provide even, effective and time-saving debridement compared to past protocols.
REGENERATION AROUND CLEANED IMPLANTS
Example using Powerbone Dental Putty (Fully adsorbing dental bone graft)

Regrafting with a fully resorbing bone regeneration material.
Immediately after re-grafting, in this case with Dental Putty, the graft particles appear dense and easy to see. Three weeks later, regeneration of new bone is underway, and the site has new vascularity, making the graft less well defined. At 3 months, mineralisation of the graft is occurring, particles are reduced in size, with graft resorption is occurring at the edges.
Loading increases bone turnover and accelerates the remodelling of fully resorbable grafts.
More thinking on at risk cases…
VITAMIN D TESTING
Studies highlight that patients with low vitamin D show early implant failure. A simple 15-minute test can be performed by clinic staff, which provides a numerically accurate (lab level) result, removing doubt and providing reassurance when scheduling revision cases.

The Spark D Vitamin D test detects Vitamin D2 and D3 in the range of 4 ng/ml – 100 ng/ml with high specificity and no interference of Biotin and is used in conjunction with a mobile phone-based app for lateral flow reading and data recording. Each test takes only 15 minutes and can be easily completed by practice staff.
Read more. An article providing more detail is available at https://restore-surgical.co.uk/increase-consent-reduce-failures/
Where can I get NiTi brushes?
https://restore-surgical.co.uk/product-category/regen-store/niti-implant-cleaning-brushes/
Where can I get fully resorbing bone grafts?
Regen Store at Restore Surgical supplies a variety of fully resorbing Powerbone graft materials some of which are ideal for mixing with antibiotics. These can be purchased online at the following link:
ask@regen-store.co.uk
References: 1. Ramanauskaite and Schwarz. Surgical Management of Peri-implantitis. Curr Oral Health Rep 7, 283–303 (2020). https://doi.org/10.1007/s40496-020-00278-y. 2. Toma S, Brecx MC, Lasserre JF. Clinical evaluation of three surgical modalities in the treatment of Peri-Implantitis: a randomized controlled clinical trial. J Clin Med. 2019;8(7):966.